Approach to
Red Eye
Sangeetha Santhakumaran1
Published online: 8 March 2021
1McGill University, Montreal, QC, Canada
Corresponding Author: Sangeetha Santhakumaran, email sangeetha.santhakumaran@mail.mcgill.ca
DOI: 10.26443/mjm.v19i1.196
Abstract
Red eye is a common symptom that presents in primary care practice, and may be accompanied by pain, irritation, or discharge. It is a sign of ocular inflammation, often involving the anterior segment of the eye. Most causes of red eye are benign; however, the primary care physician must identify when urgent referral to an ophthalmologist is required. This may be achieved through targeted questioning regarding the chronicity, intensity of pain, vision changes, and associated symptoms. The following article outlines an approach to identifying the cause of red eye using history and physical exam findings. Common features of red eye disorders and their respective treatment modalities are discussed.
Tags: Red Eye, Hyperemia, Ocular Inflammation, Conjunctivitis, Infection
Question
A 35-year old man presents to your office with a two-day history of persistent, diffuse left-eye redness. He notes watery discharge from the left eye and a mild burning sensation in both eyes with no ocular pain or foreign body sensation. Associated symptoms include rhinorrhea over the past two days.
The patient has no significant past medical history, does not take medication, and has no known allergies. He does not report increased exposure to dust, animals, or pollen. His daughter has had similar symptoms since starting daycare a few days ago.
Upon examination, both eyelids and surrounding structures are unremarkable. Examination of the left eye shows diffuse hyperemia of conjunctival vessels, scant watery secretions, and dried crusting of the eyelid. The right eye contains minimal watery secretion but is otherwise unremarkable. There is absence of corneal opacity bilaterally. Vision testing reveals no change in visual acuity. Penlight examination reveals pupils that are equal, round, and reactive to light (PERRL) and a normal anterior chamber depth. Extraocular movements are normal in all cardinal directions of gaze. Preauricular and submandibular lymph nodes are enlarged.
What is the most appropriate next step in management of this patient?
- Obtain a bacterial culture
- Refer to an ophthalmologist
- Prescribe broad-spectrum antibiotic eyedrops
- Instruct the patient to apply cool compresses and avoid sharing personal items with others (i.e. towels)
- Prescribe steroid eye drops to reduce inflammation
Answer
D) The two-day diffuse hyperemia, mild burning sensation, and associated rhinorrhea suggest conjunctivitis. A viral conjunctivitis is differentiated from bacterial conjunctivitis based on its watery rather than purulent discharge consistency and the presence of lymphadenopathy. Further, viral conjunctivitis generally lasts longer than bacterial conjunctivitis. Therefore, the patient does not require either a bacterial culture or antibiotic eyedrops. Cool compresses are helpful in reducing itching and inflammation. Viral conjunctivitis is highly contagious and transmission between individuals can arise from sharing personal items and close contact. In this scenario, the virus was likely transmitted to the patient by his daughter. Referral to an ophthalmologist is necessary if symptoms do not resolve within seven days, there is corneal involvement, or there is presence of conjunctival pseudomembranes/true membranes. Conjunctival pseudomembranes appear as thin yellowish-white membranes in the fornices of the eye. Steroid eye drops are useful in treating ocular inflammation; however, they should only be given in severe cases of conjunctivitis and under direct supervision of an ophthalmologist.
Main Text
Initial Approach
Red eye refers to hyperemia of conjunctival or episcleral vessels secondary to disease of almost any part of the eye. Most cases can be treated by a primary care physician, although a subset require urgent ocular referral. Evaluation of a patient with red eye should begin with a thorough history of ocular-related symptoms followed by a complete review of systems.
The following details are important to elicit on history. (1):
- The onset and duration of hyperemia, unilateral or bilateral eye involvement, whether it has been stable or progressively worsening, and whether it is present constantly or intermittently
- Ocular pain and its quality and severity. Ocular pain should be differentiated from itchiness or irritation
- Foreign-body sensation
- Changes in vision or photophobia
- The presence of epiphora, discharge (type and amount), pus, or blood in the eye
- Other associated symptoms (e.g. rhinorrhea, sore throat)
- Environmental exposures, close contacts with similar symptoms, and recent trauma
- Past medical history including ocular disorders, systemic disorders, sexually transmitted infections, clotting/vascular disorders, allergies, contact lens use, surgical history, and medication history
The physical examination should be completed on both eyes. Start with inspection of the eyelids and surrounding structures, assessing for swelling, erythema, or deformities. The tarsal conjunctiva should be screened for papillae or follicles, which are characteristic of allergic conjunctivitis or chlamydial conjunctivitis respectively. (2) If a foreign body is suspected, evert the eyelid using a cotton swab for further assessment. Next, the qualitative characteristics of the ocular hyperemia should be described as diffuse, localized with poorly demarcated borders, localized with well-demarcated borders, or ciliary/limbal injection. If discharge is present, it should be quantified and characterized as purulent (characteristic of bacterial conjunctivitis or keratitis), watery (characteristic of viral or allergic conjunctivitis), or mucoid (characteristic of chlamydial conjunctivitis). (1-3) The presence of pus (hypopyon) or blood (hyphema) in the anterior chamber should prompt immediate ophthalmologic referral. (1)
Visual acuity may be measured using a Snellen chart for distance acuity or a reading sample to measure near acuity (with correction). Extraocular movements are evaluated by directing the patient to look in the cardinal directions of gaze. Next, the penlight exam can reveal whether pupils are equal, round, and reactive to light (PERRL). Tonometry may be used to measure intraocular pressure; however, this should be avoided if ocular trauma is suspected. Normal intraocular pressure is 10-21 mmHg. (4) Next, opacities of the cornea may be assessed. Corneal epithelial dysfunction can be evaluated using fluorescein stain and a Wood’s or cobalt blue lamp.
Once the ocular exam is complete, an infectious disease process should be ruled out by inspection of the nose and throat and evaluation of regional lymph nodes. The remainder of the physical exam may be tailored based on suspicion of systemic or other disease.
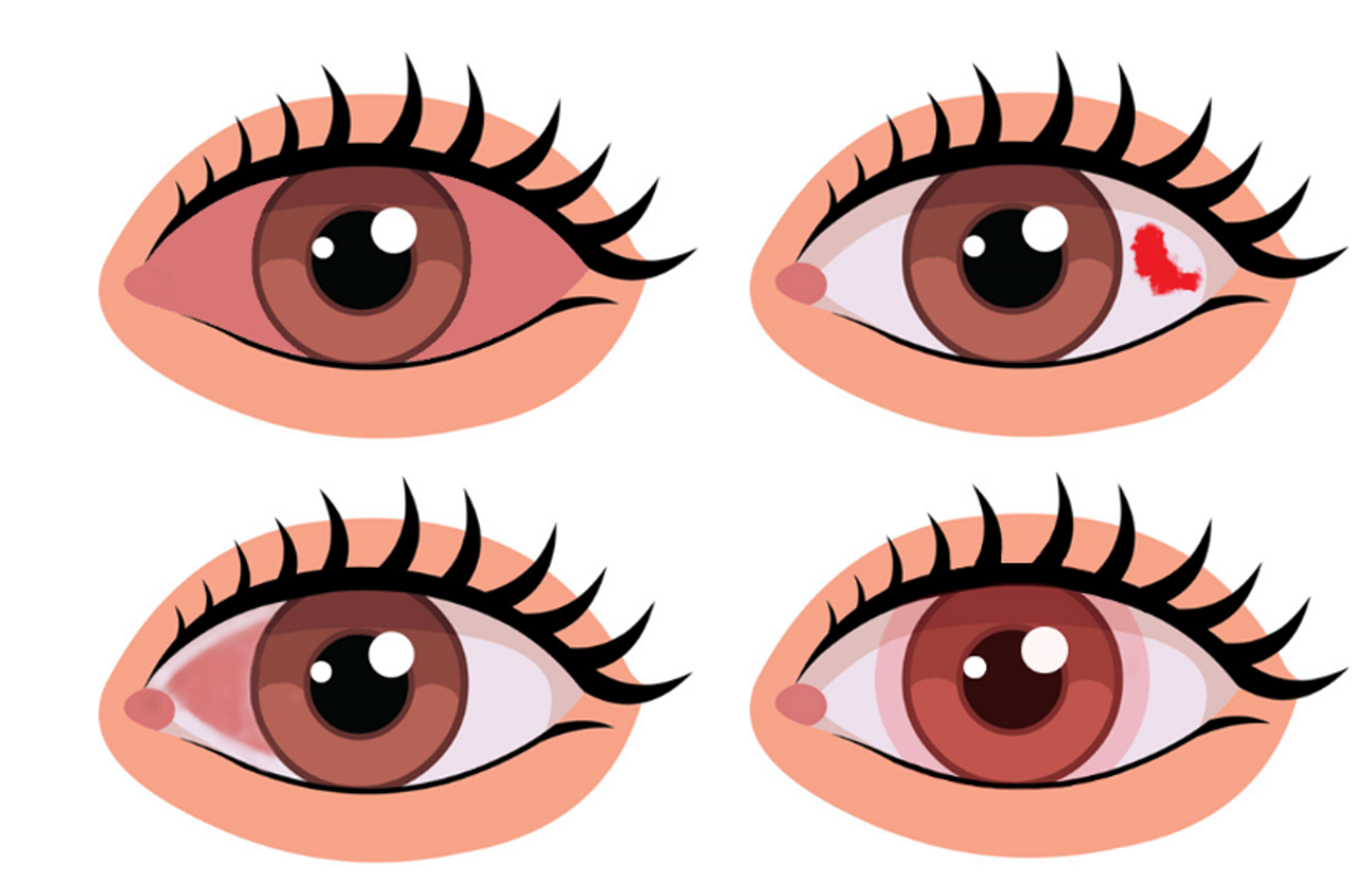
Clipart modified from Classroom Clipart. (5).
Beyond the Initial Approach
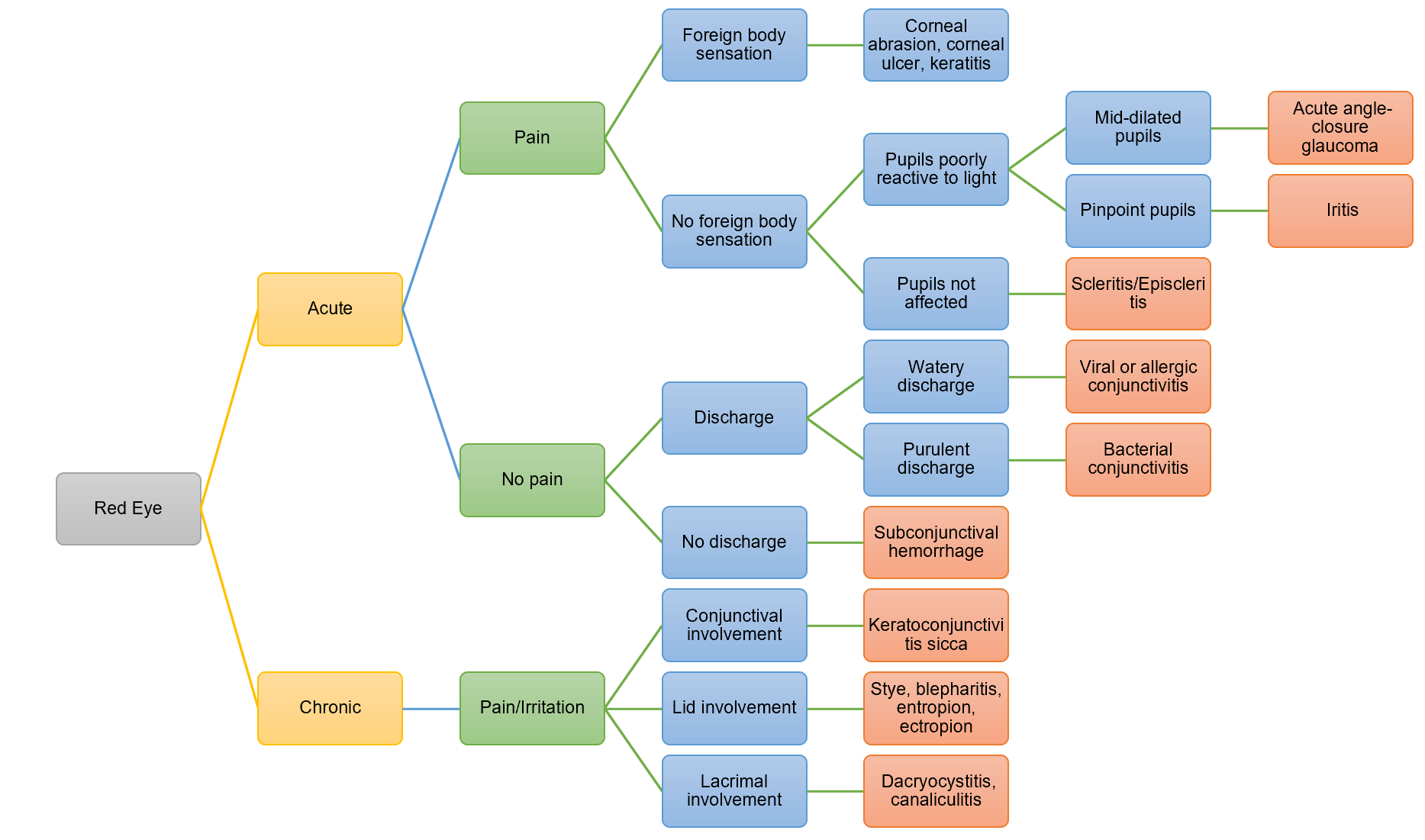
This section covers a selected number of diseases that may present with red eye, organized by the duration of symptoms and presence or absence of pain. Acute presentation is defined as a duration of symptoms for seven days or less. (3)
Acute, painful disease
Corneal abrasion occurs when there is a scratch to the cornea from contact with small particles such as dust or dirt, or direct injury from an object. (3) The patient often presents with eye pain, epiphora, and a foreign-body sensation. (3) Removal of a corneal foreign body should be completed with slit-lamp examination to avoid further corneal damage. (6) Management includes analgesics, cycloplegics, and prophylactic antibiotic therapy. (3) Individuals with chemical penetration should irrigate the eye with sterile water or saline for 20 minutes prior to emergent ophthalmologic referral. (7) Keratitis refers to infectious or non-infectious corneal inflammation. Infectious organisms may be found in contact lenses or contaminated water, and individuals with ocular injury or prolonged topical corticosteroid use are at heightened risk of infection. (1, 8) Herpes simplex keratitis is an infection caused by the HSV strain. (4, 8) Symptoms of keratitis include ocular pain and/or irritation, blurred vision, photophobia, redness, and discharge. (1) In viral keratitis, watery discharge may be present and corneal staining may reveal a dendritic pattern of the epithelium in HSV-specific keratitis. (1) In bacterial keratitis, a mucopurulent discharge is present often with corneal opacification. (1, 4) Keratitis may be treated with artificial tears for mild cases, with possible antimicrobial therapy depending on the cause. (8) Infection of the cornea may lead to a corneal ulcer, whereby there is loss of corneal tissue. (8) This finding should be immediately referred to an ophthalmologist.
Scleritis is inflammation of the sclera and may present with nocturnal ocular pain, redness, blurring of vision, photophobia, and epiphora. (3) Scleritis is often associated with underlying systemic disease such as rheumatoid arthritis or granulomatosis with polyangiitis. Management includes administration of oral non-steroidal anti-inflammatory drugs (NSAIDs), while severe cases may require treatment with oral corticosteroids. (3, 9) Episcleritis is associated with mild pain and occurs due to inflammation of the superficial episcleral vessels. (4) Episcleritis can be treated with supportive therapy such as lubricating drops, while recurrent cases can be managed with oral NSAIDs. (4, 9) Anterior uveitis refers to inflammation of the iris and ciliary body. (3) Its characteristic features include severe photophobia and engorgement of the anterior ciliary vessels which result in a “ciliary flush”. (3)
Acute angle-closure glaucoma (AACG) is a ocular emergency referring to the closure of the angle between the cornea and the irisThis impairs drainage of the aqueous humor resulting in increased intraocular pressure. (10, 11) Patients often present with severe eye pain and redness, headache, nausea, vomiting, coloured halos, mid-dilated and poorly reactive pupils, and photophobia. (4, 10) AACG treatment is directed at relieving symptoms and decreasing intraocular pressureusing oral or topical carbonic anhydrase inhibitors, topical beta-blockers, and topical alpha-2 adrenergic agonists. (4, 10) If a pupillary block is suspected, a cholinergic agent may be used. (10) After the acute attack is resolved, a laser peripheral iridotomy is completed to allow the aqueous fluid to bypass the pupil. (10)
Eyelid-related entities, such as a stye or chalazion, may result in ocular irritation and subsequent red eye. (1) A stye is the infectious inflammation of a lash follicle. (1), while a chalazion is non-infectious. (7) Both conditions are treated with a warm compress applied multiple times a day and massages of the affected eyelid. (7)
Acute, non-painful disease
Subconjunctival hemorrhage is the bursting of a conjunctival blood vessel, which causes blood to leak between the conjunctiva and sclera. (3) Patients present with a bright red spot in the sclera. (12) Subconjunctival hemorrhage may occur in response to a Valsalva maneuver (coughing, straining) and is more common in individuals with cardiovascular disease or bleeding disorders. (3, 11)
Conjunctivitis refers to dilatation of the small blood vessels within the conjunctiva. (3, 12) It may be due to infection, allergy, or irritants. (3) The most common form of conjunctivitis is caused by adenovirus and is contagious. (3) Viral conjunctivitis generally starts unilaterally and progressively infects the other eye. (2) Laboratory tests are warranted in resistant cases of bacterial conjunctivitis or in immunocompromised patients. (7, 12) Both viral and bacterial conjunctivitis are treated with rigorous hygiene and the application of a cool compress. (7) Bacterial conjunctivitis is additionally treated with antibiotic eyedrops. (3) Allergic conjunctivitis generally presents with bilateral tearing and causes eye itchiness. (3) It may be treated with an over-the-counter antihistamine. (3)
Chronic, painful/irritating disease
Keratoconjunctivitis sicca, or dry eye, can be caused by multiple etiologies, including decreased tear production, increased tear evaporation, or imbalances in the mixture of water, oils, and mucus in the tear film. (3) Patients may feel a foreign body sensation and generalized ocular irritation with paradoxical tearing. Precipitating factors include anticholinergic and antihistamine medications, increased age, and medical conditions such as rheumatoid arthritis, diabetes, and Sjogren’s syndrome. (3) Mild keratoconjunctivitis sicca may be treated with artificial tears, lubricant ointments, and the usage of humidifiers. (3)
Blepharitis is a chronic inflammation of the eyelid. The patient presents with itchy, inflamed, crusted eyelids with misaligned eyelashes. (13) Anterior blepharitis may occur due to staphylococcal infection or seborrheic dermatitis. (13) Posterior blepharitis, the more common presentation, may occur due to clogging of the meibomian glands or inflammatory skin conditions such as rosacea. (13) Both are treated through eyelid hygiene using eyelid wipes, a warm compress, an eyelid scrub, diluted baby shampoo, and, in select cases, an antibiotic ointment. (7, 13) Ectropion is eversion of the eyelid which renders the eye prone to irritation. (14) Entropion is inversion of the eyelid which can cause the eyelashes to strike the cornea. (14) Symptoms of ocular irritation are generally treated using eyedrops; however, surgery is required for complete correction. (14).
As a non-specialist, it is important to recognize immediate referral is required. These include reduced visual acuity, severe ocular pain, photophobia, corneal opacification or epithelial dysfunction, pupillary abnormalities, hypopyon, and hyphema. (2, 7) Timely referral is crucial in preventing sight-threatening complications.
| Table 1: Presence of ocular signs in red eye disorders | Disease | Severe pain | Irritation | Foreign body sensation | Epiphora | Discharge | Photophobia | Reduced acuity |
| Acute angle-closure glaucoma | X | X | X | X | |||
| Conjunctivitis | X | X | |||||
| Corneal abrasion | X | X | X | X | X | ||
| Corneal ulcer | X | X | X | X | X | X | |
| Episcleritis | X | X | |||||
| Iritis | X | X | X | ||||
| Keratitis | X | X | X | X | X | ||
| Keratoconjunctivitis sicca | X | X | X | ||||
| Scleritis | X | X | X | X | |||
| Subconjunctival hemorrhage | |||||||
Adapted from:. (4, 11, 12)
*X indicates presence of the stated characteristic
References
- Heidelbaugh JJ. Primary Care Ophthalmology, An Issue of Primary Care: Clinics in Office Practice 42-3, E-Book: Elsevier Health Sciences; 2015 [cited 2021 Feb 13].
- Smith J, Severn P, Clarke L. Evaluation of red eye. 2018. In: BMJ Best Practice [Internet]. London: BMJ Publishing Group.
- Cronau H, Kankanala RR, Mauger T. Diagnosis and management of red eye in primary care. American Family Physician. 2010;81(2):137-44.
- Jacobs D. Overview of the red eye. In: Gardiner M, Givens J, editors. UpToDate. Waltham, MA: Wolters Kluwer; 2020 [cited 2021 Feb 13].
- Classroom Clipart. Human Eye Clipart. 2020.
- Merck Manuals [Internet]. How to Remove a Foreign Body from the Eye. Merck Sharp & Dohme Corp. 2020 [cited 2021 Feb 13]. Available from: https://www.merckmanuals.com/en-ca/professional/eye-disorders/how-to-do-eye-procedures/how-to-remove-a-foreign-body-from-the-eye.
- Harper RA. Basic ophthalmology. Ninth edition. ed. San Francisco, CA: American Academy of Ophthalmology; 2010.
- Mayo Clinic Staff. Keratitis Rochester, Minnesota: Mayo Foundation for Medical Education and Research; 2020 [updated August 28, 2020; cited 2020]. Available from: https://www.mayoclinic.org/diseases-conditions/keratitis/ symptoms-causes/syc-20374110.
- Diaz JD, Sobol EK, Gritz DC. Treatment and management of scleral disorders. Survey of Ophthalmology. 2016;61(6):702-17.
- Prum BE, Herndon LW, Moroi SE, Mansberger SL, Stein JD, Lim MC, et al. Primary angle closure preferred practice Pattern® guidelines. Ophthalmology. 2016;123(1):P1-P40.
- Frings A, Geerling G, Schargus M. Red Eye: A Guide for Non-specialists. Dtsch Arztebl Int. 2017;114(17):302-12.
- Leibowitz HM. The red eye. New England Journal of Medicine. 2000;343(5):345-51.
- Bernardes TF, Bonfioli AA. Blepharitis. Seminars in Ophthalmology. 2010;25(3):79-83.
- Vallabhanath P, Carter SR. Ectropion and entropion. Current Opinion in Ophthalmology. 2000;11(5):345-51.

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.